마네킨 연구에서 손힘과 가슴압박과의 연관성
Relationship between Hand Force and Chest Compression in Manikin Study
Article information
Abstract
요 약
요 약 영아 심정지에서 두 손가락을 이용하여 가슴압박(Two-finger chest compression technique)을 시행할 경우 가늘고 긴 손가락일수록 C자형으로 굽어짐이 발생된다. 이로 인해 수직으로 가슴압박을 하는 것이 쉽지 않다. 이 연구는 심정지 영아에서 악력과 배근력이 가슴압박의 결과에 영향을 미치는지를 알아보기 위한 마네킨 실험이다. 실험대상은 심폐소생술을 15주 이수한 응급구조학과 4학년 학생 20명으로 하였다. 연구결과 남자가 여자보다 악력이 높게 나타났으며, 악력과 키, 성별이 가슴압박의 깊이에 유의한 관계를 보였다. 두 손가락을 이용한 가슴압박은 시간이 경과할수록 압박깊이가 감소되었고, 불완전 이완율이 높게 나타났다. 시간 경과에 따라 압박 깊이를 유지하기 위해서는 악력이 영향을 미치는 것으로 나타났으며, 기초체력 향상을 위한 프로그램이 필요할 것으로 판단된다.
Trans Abstract
ABSTRACT
A C-shaped bend is prevalent in long, thin fingers when administering the two-finger compression technique in infant cardiac arrest, making vertical chest compressions difficult. This study was a mannequin experiment, which investigated the effect of grip and back muscle strengths on the outcome of infant chest compressions. Twenty 4th year paramedicine students who had completed 15 weeks of cardiopulmonary resuscitation (CPR) training were recruited as subjects in this study. The results demonstrated greater grip strength in men than in women. Additionally, grip strength, height, and sex were found to have significant correlations with the depth of chest compressions. The chest compression depth decreased over time, using the two-finger compression technique, while the rate of incomplete release increased. Grip strength was observed to affect the ability to maintain compression depth over time, demonstrating the need for a program to improve basic fitness.
1. Introduction
Compression depth and release should be maintained consistently so that it can increase the systolic and diastolic pressure. In performing chest compression using two fingers, vertical compression is not easy and longer and thinner fingers are likely to bend as c-shape. Thus, it is difficult to perform compression by one third of chest depth or 4 cm.
Appropriate chest compression depth in cardiac arrest in pre-hospital admission is one of the most important factors in improving survival rate(1,2). In order to achieve effective chest compression in infants' cardiac arrest, survival rate can be improved only when the position of the chest compressions, compression speed and depth, and complete release after compression are all achieved. When rapid and accurate chest compressions are performed, there is a higher chance of return of spontaneous circulation and lower chance of neurological sequelae.
Although the infant mortality rate in Korea is low compared to other OECD Member countries at a rate of 2.8 infant deaths, there was an increase of 4.7%(0.1 infant deaths) in 2016(3). The rate of cardiac arrest in infants and children is approximately 70 out of 100,000, out of which 28.8% can be attributed to infant cardiac arrest. 70% of cardiac arrest happens at home and 37.1% is witnessed. Spontaneous circulation recovery of witnessed cardiac arrest is 5.5%, with a Cerebral Performance Categories Scale (CPC scale) of 1,2 in 3.7% of cases(4).
According to American Heart Association (AHA) and Korean Association of Cardiopulmonary Resuscitation (KACPR) in 2015(3,4), when performing compression in infant cardiac arrest patient, compression should be done using two fingers or two thumbs on the area just below the point where the virtual line connecting the both nipples and the sternum meets. Compression speed should be maintained at 100∼120 per min, and care should be taken not to compress the xiphoid and ribs. Compression should be done by at least one third of chest depth or 4 cm.
According to the previous study, depth of chest compression did not exceed 3 cm in the group without finger support and the depth decreased more especially after 5 min(5). Two-thumb chest compression technique increases more coronary perfusion pressure compared to two-finger compression, providing more blood to the heart muscle. In addition, as the depth of chest compression is maintained consistently, blood pressure of arterial blood can be maintained higher.
This study aimed to analyze the compression depth in two-finger compression technique during single-rescuer infant CPR according to the AHA guidelines and compare it with grip strength to collectively investigate changes in chest compression depth in relation to grip strength.
2. Proposed Method
2.1 Study design
Unlike adults and children, hand strength, especially finger strength, can affect the quality of chest compressions in infants. This study is a mannequin experiment to investigate whether grip affect chest compression in infant. The subjects of this study were 20 fourth grade students of the emergency medical services department who completed 15 weeks of CPR course. First, the grip strength of both hands were measured. My-5401 (TAKEI, Japan) was used for measurement of grip strength. Chest compressions were conducted based on the infant CPR Guideline by American Heart Association (AHA).
In the experiment, chest compressions were performed for 10 min while two participants in one group taking turns every 2 min. Experimental method consisted of two-finger compression.
2.2 Experiment equipment
2.2.1 Simulator
Resusci Baby QCPR (Laerdal medical, Stavanger, Norway) and SimPad were used as mannequin. The mannequin enabled chest compressions and intubation and, paired with a software program, SimPad PLUS with SkillReporter (Laerdal, Stavanger, Norway) enabled measurements of chest compression depth, speed, location, incomplete release, and time at which compressions were terminated, as well as the collection of more specific data, such as the amount of oxygen delivered to lungs, speed, and breath cycle during mouth-to-mouth ventilation.
2.2.2 Grip strength
A my-5401 (TAKEI, Japan) digital grip strength tester was used to measure grip strength of both hands, 3 time each, for a total of 6 measurements, and a questionnaire was administered regarding the dominant hand (Right or left). In this study, the grip strength of the dominant hand was primarily used for analysis.
2.3 Analysis
The study was conducted from August 1, 2019 to August 15, 2019. After loading data saved in SimPad, comDepth, compReleaseDepth, comLeaningDepth, were collected in text file. Organization and statistical analysis of the collected data was done using SPSS (v 20.0 SPSS Inc., Chicago, USA.). Frequency analysis and t-test were performed on depth of chest compression, depth of incomplete release, minimum time between chest compressions, and variables in measurement results, while a Chi-square test was used to compare the accuracy of hand location during chest compression between the two groups and analyze the number of incomplete compressions.
3. Experimental Results
3.1 personal characteristics
20 subjects participated in the study, comprised of 10 men and 10 women. The characteristics of the men and women were as follows: an average age of 22.9 years for men and 21.4 years for women; an average weight of 71.59 kg for men and 57.18 for women; an average height of 173.40 cm for men and 162.70 cm for women; an average grip strength of 44.33 kg for men and 28.87 kg for women; and an average compression depth of 43.31 mm for men and 43.00 mm for women (Table 1).

Personal Characteristics
3.2 Compression depth
Chest compressions were performed in 5 groups, one group consisted of two men and two women. The average compression depths in male groups were: 43.76 ± .44 mm in group 1; 39.71 ± 2.34 mm in group 2; 43.25 ± .21 mm in group 3; 43.09 ± 1.04 mm in group 4; and 42.68 ± .85 mm in group 5. The average compression depths in female groups were: 42.44 ± 1.24 mm in group 6; 39.39 ± 3.98 mm in group 7; 39.68 ± 4.20 mm in group 8; 39.56 ± 2.51 mm in group 9; and 39.71 ± 2.53 mm in group 10. The average chest compression depth across all groups was 41.34 mm, while the average compression depth in male groups was 43.70 ± .44 mm and the average compression depth in female groups was 39.71 ± 2.34 mm (p = .000) (Table 2)
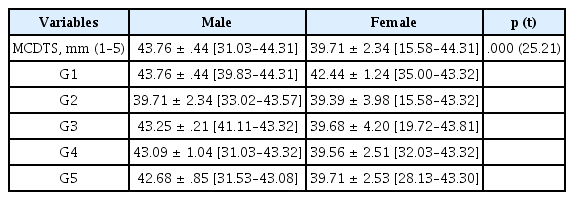
Results of Compression Depth and Rate
When chest compression depth is classified to the nearest 10 mm after 10 min of chest compressions, a difference can be observed (Table 2). Compared to the male groups, where 88.56% of the compressions were done to a depth of 4∼4.5 cm and 11.44% to a depth of 3∼3.99 cm, the female groups had 59.95% of the compressions done to a depth of 4∼4.5 cm, 39.05% to a depth of 3∼3.99 cm, .82% to a depth of 2∼2.99 cm and .18% to a depth under 2 cm (Table 3, Fig. 1.).

Results of Chest Compression Depth (%)
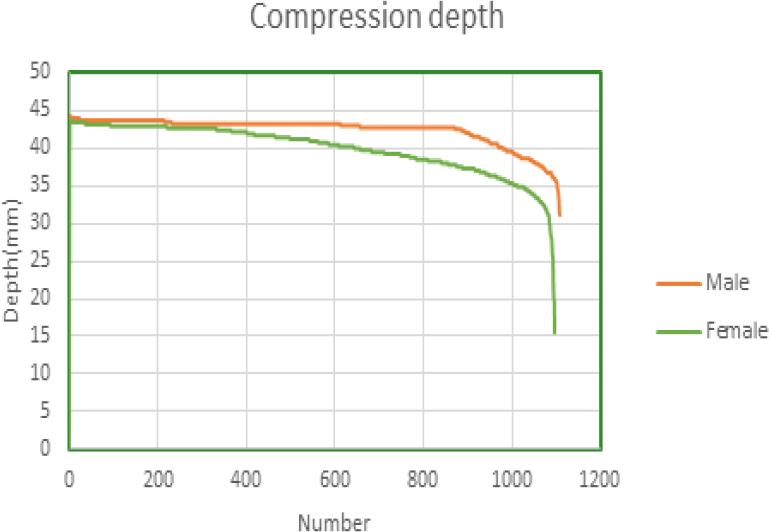
Comparison of chest compression over time.
3.3 Comparison of release depth
As normal release following a compression is considered within a 5 mm range of errors, a value greater than 5 mm was classified as incomplete release. A release depth of 2.11 ± 1.55 mm in men and 2.75 ± 1.34 mm in women (p = .000). Upon examination of the rate of incomplete release based on a 5 mm range of errors, men demonstrated 75 cases of incomplete release at a rate of 6.77%, and women demonstrated 81 cases of incomplete release at a range of 7.40% (Table 4).

Comparison of Release Depth
3.4 Minimum depth between current and next compression
The minimum depth between compressions is an index to determine the consistency of chest compressions. The average minimum depth observed in men was 2.10 ± 1.55 mm and 2.74 ± 1.34 mm in women (p = .000)(Table 5, Fig. 2.).

Minimum Depth between Current and Next Compression
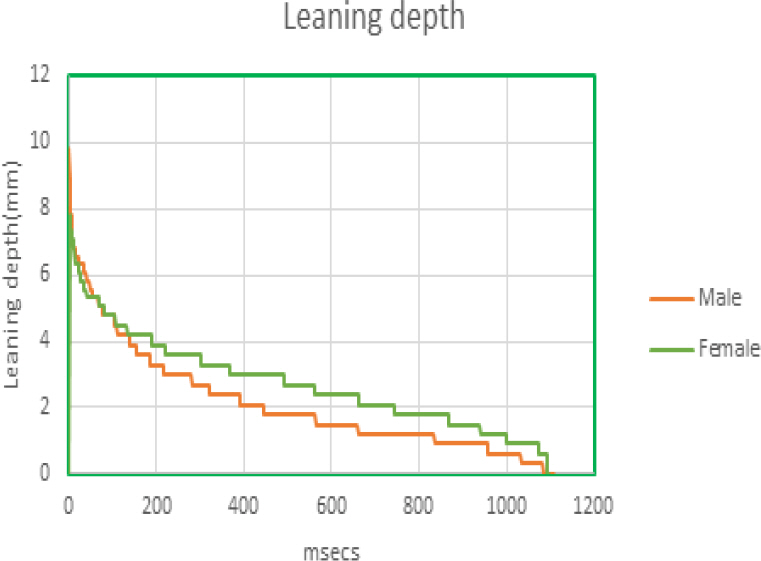
Minimum depth between current and next compression.
3.5 Correlation between personal characteristics and compression depth
Grip strength and height demonstrated a significant positive correlation with chest compression depth, while sex demonstrated a significant negative correlation. Compression depth increased with greater grip strength and height (Table 6).

Correlation of Personal Characteristics and Compression Depth
4. Discussion
High quality chest compressions are the most important component of resuscitation. High quality chest compressions require maintenance and consistency in compression depth, location, speed, and complete release. The anatomical finger length and strength of the rescuer may affect the maintenance of vertical fingers during infant chest compressions. Women, especially, who tend to have long, thin, fingers, may easily become fatigued while trying to apply force or support. This study is a basic research exploring the effect of grip strength and personal characteristics on the quality of chest compressions.
Compression depth for two-finger chest compression technique for men and women were 43.31 mm and 43.00 mm, respectively. Previous research using meta-analysis indicated compression depths of 2.2∼2.6 cm(8–10) and 3.9 cm(11,12). Such differences demonstrated that using two fingers rather than two thumbs lowered the depth of compressions in infant chest compressions. Furthermore, mannequins were used in Lee and Jiang et al.(11,12), and it has thus been presumed that chest compression depth varied depending on the characteristics of the rescuer. 4th year university students were selected as subjects for this study. Differences from previous studies may have arisen due to the fact that the subjects in this study had completed a 15-week BLS course in their 1st year and attended two 7-week clinical trainings in hospital.
There was no significant difference in chest compression depth between men and women. However, when compared to the nearest 10 mm, 88.56% of the chest compressions done by men had a depth of 4∼4.5 cm and 11.44% had a depth of 3∼3.99 cm, whereas for women, 59.95% of chest compressions were done to a depth of 4∼4.5 cm, 39.05% were done to a depth of 3∼3.99 cm, and 1.0% was done to a depth under 2.99 cm. This difference was attributed to the fact that women, more than men, tended to lose compression depth over time. Furthermore, there were 75 cases of incomplete release in men, at a rate of 6.77%, compared to 81 cases of incomplete release in women, at a rate of 7.40%. A similar difference was observed in grip strength, with men demonstrating greater grip strength than women, where greater strength indicated a better maintenance of compression depth. Rescuer weight was found not to have an effect on compression depth, although rescuer height had an effect if the chest compressions were performed in a kneeling position. In adults, however, weight was found to have an effect(13,14). Even in infants, different results may be observed depending on the experimental method.
A limitation of this study is that clinical applications and generalization may be difficult, due to the recruitment of undergraduate students from a single university as study subjects, not to mention the use of mannequins. Further qualitative research on chest compressions with consideration of basic physical strength will be necessary, given that components of basic physical strength other than grip strength were not included in this study.
5. Conclusion
This study aimed to explore factors that affected the quality of chest compressions over time. Results indicated higher grip strength in men compared to women, and a significant correlation between chest compression depth and grip strength, height, and sex. Chest compression depth when using the two-finger compression technique decreased with time, while incomplete release increased. Grip strength was observed to have an effect in maintaining compression depth over time, indicating a need for a program to improve basic physical strength.