수평피난안전구역 설치여부에 따른 노인요양병원의 화재위험평가
Evaluating Fire Risk of Long-term Care Hospitals for the Elderly
Article information
Trans Abstract
ABSTRACT
Long-term care hospitals for the elderly have a high risk of fire. To reduce this risk, the installation of a horizontal refuge area has been stipulated since 2015. However, most hospitals are still at risk due to the lack of retroactive regulations. Therefore, in this study, the efficiency of the horizontal refuge area was analyzed through evacuation safety evaluation using fire and evacuation simulations. As a result of evacuation safety evaluation for the two hospitals, the reduction ratio of evacuation time was 70% (day time) and 77% (night time). In addition, evacuation safety can be secured through the installation of a horizontal refuge area. The results of this study are expected to be used as a basis for preparing retroactive regulations for horizontal refuge areas in long-term care hospitals for the elderly in the future.
Introduction
1.1 Background and Purpose of the Study
The elderly and patients with impaired mobility are cared for in long-term care hospitals. However, the possibility of occurrence of damage in these hospitals is very high in the event of a fire because of the low walking speeds of patients and the challenges of transporting patients in bed (moved by evacuation assisters using stretchers and rescue hoses).
To reduce the risk of long-term care hospitals for the elderly, the Korean government made some stipulations. Article 46 (6) of the Enforcement Decree of the Building Act has stipulated measures such as the installation of fire-partitioned evacuation spaces, evacuation balconies, and connecting pathways on each floor from 2015. In this paper, these measures are collectively referred to as horizontal refuge areas. However, since there is no retroactive provision on buildings completed and permitted before the amendment of the law, the majority of long-term care hospitals for the elderly are still exposed to danger.
Therefore, this study intends to prove the efficiency of the horizontal refuge areas designated for long-term care hospitals for the elderly through fire and evacuation simulations and present the rationale for preparing retrospective provisions.
1.2 Scope and Methods of the Study
In this study, fire and evacuation simulations were performed for two elderly long-term care hospitals in Gyeongnam. Evacuation safety was evaluated according to whether there were horizontal refuge areas.
First, before the simulations, the characteristics of the buildings and the actual states of hospitalization of occupants at each floor were reviewed through field surveys to select the horizontal refuge areas of each long-term care hospital for the elderly. Based on the foregoing, fire simulations (Pyrosim Mar. 2021), evacuation simulations (Pathfinder Mar. 2021), and the time of fire (daytime and nighttime) were selected as variables. Fire simulations assumed a fire that occurred in the kitchen on the first floor, while evacuation simulations were considered with four scenarios in which a horizontal refuge area was installed.
Finally, based on the results of the fire and evacuation simulations, evacuation safety evaluation was conducted according to the life safety standards of “performance-oriented design methods and standards for firefighting facilities, etc.” We considered the evaluation results of evacuation safety according to whether there were horizontal refuge areas.
2. Need for Horizontal Refuge Areas in Long-term Care Hospitals for the Elderly
In the case of hospitals, evacuation safety can be improved by minimizing the time until final evacuation is achieved in long-term care hospitals for the elderly.
The US NFPA101 Life Safety Code (Chapter 18, Chapter 19) induces horizontal evacuation in the case of nursing hospitals and stipulates that evacuation spaces should be installed in the buildings. In addition, the foregoing safety code explains that moving or evacuating all patients from the medical space is the last measure to be taken among emergency measures. It shows fire doors in cross corridors as an example of a part of a “defense in the field” protection strategy that limits the growth and spread of fire to the inside of the ignition space and reduces the necessity of evacuation of residents. When closed, the fire doors are separate fire preventive blocks from the adjacent rooms to form fire compartments, which can prevent the spread of flames, thereby playing the role of evacuation spaces(1).
In the case of South Korea, Article 46 of the Enforcement Decree of the Building Act, which is a provision newly established on September 22, 2015, stipulates that separate fire-partitioned evacuation spaces, evacuation balconies that are directly connected to the living rooms and open to the outside air, or structures in the form of viaducts installed to enable horizontal evacuation to the ground surface outside of the building or to an adjacent building should be installed on every floor. However, since this provision applies to cases where building permits or usage change permits were applied for later than September 22, 2015, there is no legal regulation on evacuation spaces for buildings completed or permitted before the amendment of the Act.
3. Evacuation Safety Evaluation Scenario
3.1 Overview of Fire and Evacuation Simulation Target Sites
In this study, two long-term care hospitals for the elderly with similar structures and numbers of beds were randomly selected to evaluate their evacuation safety by following the designation of horizontal refuge areas. The individual long-term care hospitals for the elderly were located in K and Y cities, respectively. An overview of the long-term care hospitals for the elderly is shown in Table 1.

Target Long-term Care Hospital Overview
As per the field survey results, the numbers of patients and workers in the two long-term care hospitals for the elderly are shown in Tables 2 and 3. Although the numbers of patients in the two hospitals were similar, the number of critically ill patients (those unable to walk) in the long-term care hospital for the elderly in Y city (referred to as Y hospital hereinafter) was 72, greater than that in the long-term care hospitals for the elderly in K city (referred to as K hospital hereinafter), which was 24. In addition, it was found that both hospitals divided patients into critically ill patients (impossible to walk), moderately ill patients (can walk with help or use a wheelchair), and general patients (can walk independently).

The Number of Patients

The Number of Hospital Workers
When the number of workers in individual hospitals was examined, it was found that 66 workers (male: 6, female: 60) were working at K hospital during the day, and the ratio of women was 91%. In addition, 20 workers (male: 2, female: 18) were working at night, and 90% were female. In the case of Y hospital, where there were many critically ill patients, 100 workers (male: 14, female: 86) worked during the day, and the ratio of females was 86%. In addition, 74 workers (male: 10, female: 64) worked at night) worked at night.
3.2 Selection of Evacuation Simulation Scenarios
The evacuation simulation scenarios were divided into four scenarios according to whether there was a horizontal refuge area, and the time of fire occurrence as variables, as shown in Table 4.

Case of Scenario
When horizontal refuge areas were designated (scenarios 1 and 2), a situation in which all patients were evacuated to the horizontal refuge areas on each floor was assumed. In scenarios where no horizontal refuge area was designated as with the long-term care hospitals for the elderly selected in this study (Scenario 3 and Scenario 4), simulations were performed, assuming that all patients were evacuated to the outside of the building using stairs. In addition, the number of day and night workers was applied according to the time of fire when the simulations were performed.
The horizontal refuge areas of individual long-term care hospitals for the elderly, which are the exits in the evacuation simulation, were selected by analyzing architectural features and interviews with firefighters. In the case of K hospital, although there was an exit from the hospital room on the second floor to the outside, the survey revealed that the current door width was insufficient for a bed to come out. Therefore, in this study, a plan to expand the width of the current door and select it as a horizontal refuge area was considered. In the case of the third floor, the rooftop was selected as a horizontal refuge area because there was an exit through which evacuation to the roof of the building was possible.
In the case of Y hospital, unlike K hospital, since it was impossible to designate any horizontal refuge area through which evacuation to the outside was possible, horizontal refuge areas had to be designated within the building. Therefore, in this study, additional installation of fire preventive blocks and designation of horizontal refuge areas through fire doors, which are the most easily applicable methods to existing long-term care hospitals for the elderly was considered. The study also considered the most efficient methods to implement an “on-site defense” protection strategy that minimizes the necessity of evacuation of residents. The horizontal refuge areas of the two hospitals selected according to the conditions are shown in Figure 1.

Area of horizontal refuge.
The walking speeds of individual agents selected based on the results of previous studies are listed in Table 5. The walking speeds of those workers (doctors, nurses, caregivers, etc.) that play the role of evacuation assistants were set as 1.2 m/s for men and 1.1 m/s for women based on the results of previous studies(2). Regarding walking speeds on stairs, based on the results of previous studies, 40% of the walking speed was applied when going up the stairs and 60% of the walking speed was applied when going down the stairs(3). In addition, the walking speed, preparation time for movement, and the number of persons who needed assistance for all patients were applied, as shown in Table 5, referring to previous studies(4-8).

Input Data of Walking Speed


The evacuation delay time in the fire room in the evacuation simulation was set as the detector detection time (43 s) in the case of K hospital, where the detection time of the fire detector was longer than 30 s, and was set to 30 s, which is a long time, considering the worst-case between the Japanese architectural disaster prevention formula aT0 = 2√A1) (at least 30 seconds)(at least 30 s) and the fire detector detection time (19.8 s) in the case of Y hospital. In addition, the evacuation delay time in the non-fire room was calculated by adding the reaction time to the evacuation start time in the fire room. In this study, the reaction time was calculated as 180 s because the simulations correspond to W1 of the performance-oriented design method and standard (cases where voice guidelines that can be recognized by all residents in the relevant space can be provided by trained staff members)(Table 6).

Input Data of Response Time
The locations of the occupants were set based on the results of the field survey, and the evacuation priorities of the patients were set in the order of general patients, moderately ill patients, and critically ill patients when the simulations were performed.
3.3 Selection of Fire Simulation Scenarios
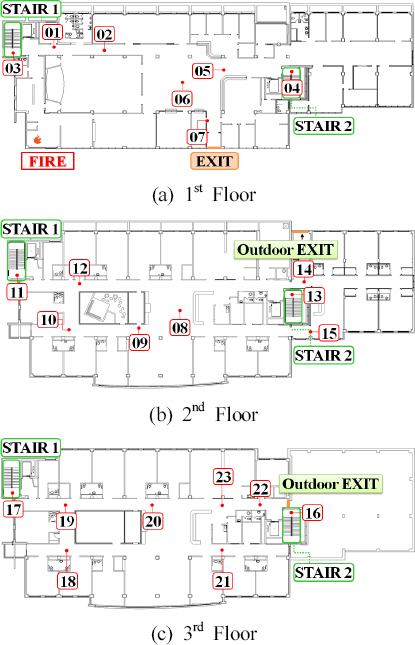
The target spaces in the two long-term care hospitals for the elderly are constructed with two evacuation stairs. We assumed a scenario in which the fire starts as small fire in the kitchen on the first floor that does not fall within the operating range of firefighting facilities but can cause a large fire (Figure 2). In addition, the initial temperature of the target spaces was assumed to be 20 °C, and the scenario was established so that the door of the fire room was open and the sprinkler facilities did not operate when the fire occurred. The fire source was assumed to be a refrigerator, the maximum heat release rate was set to 3,051 kW, and the fire growth rate was set as the medium growth rate. The size of the applied grid was set to 0.2 m × 0.2 m × 0.2 m for both long-term care hospitals for the elderly, and the total numbers of grids were set to 2,621,517 for K hospital and 2,063,016 for Y hospital when the simulations were performed (Table 7).

Location of fire.
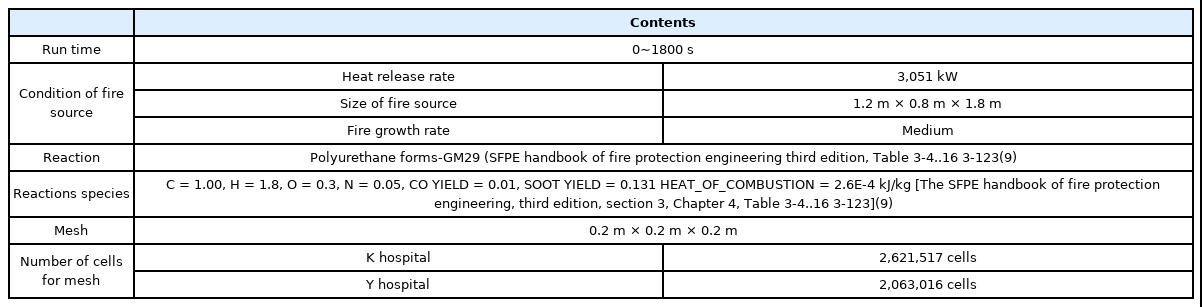
Fire Simulation Input Data
The fourth and higher floors of each building were excluded from the simulations because they did not have any hospital room. Finally, the simulations were conducted for the ignition floor (1st floor) and the three floors immediately above it (staircases in the 2nd to 4th floors and rooms in the 2nd to 3rd floors where there were patients).
4. Results of the Evaluation of Evacuation Safety
4.1 Method of Evaluation of Evacuation Safety
In this study, the evacuation safety of occupants was evaluated in the event of evacuation based on the standards for the safety of life safety of occupants presented in the “performance-oriented design methods and standards for firefighting facilities.”
To this end, heat, visibility, and toxic gases were analyzed for a plane 1.8m above the floor, which is the breathing limit of evacuees. The available safe egress time (ASET) was judged based on the life safety standards (Table 8) of “performance- oriented design methods and standards for firefighting facilities.” The required safe egress time (RSET) of occupants was analyzed through the results of evacuation simulations. It was judged that evacuation safety performance could not be secured in cases where ASET was smaller than RSET. The evacuation safety evaluation was performed on the first floor of the hospital and the entire section of the hospital rooms through the semi-coupling method. The selection of points for numerical comparison is shown in Figures 3 and 4. The points selected were the final entrance of each room, staircases, and hallways, and 23 points were selected in the case of K hospital and 26 points in the case of Y hospital.

Life Safety Standards
Location of the specific points (K hospital).

Location of the specific points on the floor plan of the studio flat at the Y hospital.
4.2 Results of Evaluation of Evacuation Safety
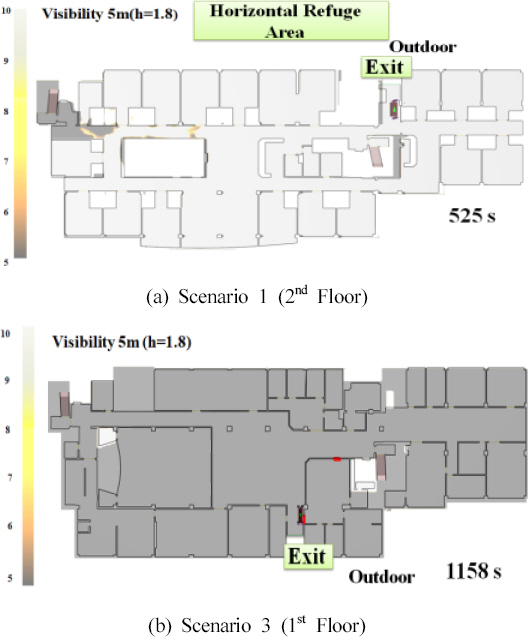
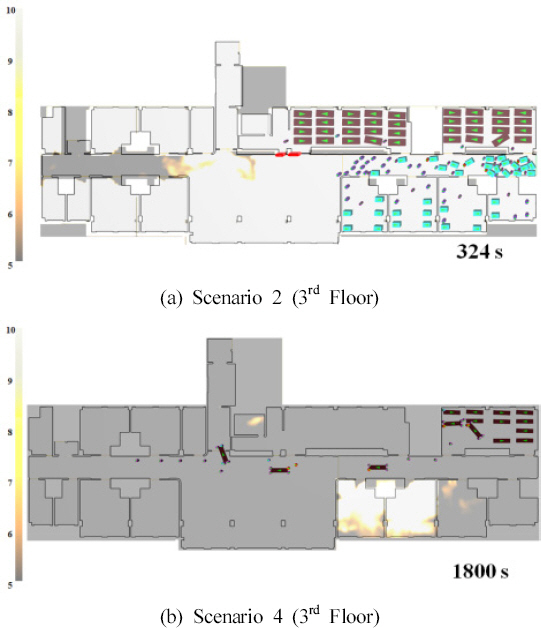
Examples of the results of semi-coupling of fire and evacuation simulations by scenario (scenarios 1-4) of K and Y hospitals are shown in Figures 5 and 6. When scenarios 1 and 3, where K hospital conducts daytime evacuation, were compared, it was identified that in the case of scenario 1, the evacuation time of the patient who passed through the outdoor exit (horizontal refuge area) on the second floor was 525 s. In contrast, in scenario 3, the last patient evacuated to the first floor at 1,158 s (Figure 5). In addition, for scenarios 2 and 4, in which the Y hospital evacuated at night, the evacuation time of Scenario 2, in which patients evacuated to the horizontal refuge area (fire compartment), was 324 s,. In contrast, the evacuation from the 3rd floor was not completed even at 1800 s, which is the simulation execution time, in scenario 4 (Figure 6).
Scene of Fire and evacuation semi-coupling at the K hospital.
Scene of fire and evacuation semi-coupling at the Y hospital.
The evaluation results of ASET, RSET, and evacuation safety of individual points in the two hospitals selected as mentioned above are shown in Table 9. In this case, ASET was determined based on the value (visibility) that reached the safety standard first among heat, visibility, and toxic gases.

Results of Evacuation Safety Assessments Using Pyrosim and Pathfinder at the K & Y Hospital
The RSETs of K and Y hospitals were compared based on whether the horizontal refuge areas were designated. In cases where horizontal refuge areas were designated (Scenario 1), the maximum RSET in the daytime when many workers work was shown to be 520 s in the case of K hospital (point 14) and 340 seconds in the case of Y hospital (point 15). In addition, in cases where no horizontal refuge area was designated (Scenario 3), it was shown to be 1158 s for K hospital (point 7) and 2174 s for Y hospital (point 6). That is, when the horizontal refuge areas were designated, the RSET reduction rate was 55% in the case of K hospital and 84% in the case of Y hospital during the daytime. In the case of night, when fewer workers work compared to the daytime, the maximum RSET was shown to be 747 seconds in the case of K hospital and 326 seconds in case Y hospital when horizontal refuge areas were designated (Scenario 2), and 2353 s in the case of K hospital and 2311 seconds in case Y hospital when no horizontal refuge area was designated (Scenario 4). Therefore, when the horizontal refuge area was designated, the reduction rate of RSET was 68% in the case of K hospital and 86% in the case of Y hospital.
Scenario 1, which is the best scenario, and scenario 4, which is the worst scenario, were compared. In scenario 1, in which evacuation safety areas were designated and evacuation was carried out in the daytime, the increased rate of RSET was shown to be 353% in the case of K hospital. In scenario 4, in which no evacuation safety area was designated and evacuation was carried out at night, the increased rate of RSET was 580% in the case of Y hospital.
According to the evaluation of evacuation safety results, in the cases of scenarios 1 and 2 where the horizontal refuge areas were designated, the ASET was higher than the RSET at all points, indicating that evacuation safety was secured. However, in the case of scenarios 3 and 4, where the horizontal refuge area was not designated, it was found that evacuation safety was not secured at most points both during the daytime and at night, and the difference between ASET and RSET was shown to be larger at night on average (K hospital: daytime 48 s, night 580 s, Y hospital; daytime 1456 s, night 1639 s).
In other words, the simulation results show that when horizontal refuge areas are installed, evacuation safety can be secured both during the daytime and at night. When no horizontal refuge area is installed, more casualties can occur at night than during the daytime.
5. Conclusion
To reduce the risk of fire for long-term care hospitals for the elderly, the installation of horizontal refuge areas has been stipulated since 2015. However, due to the absence of retroactive provisions, the majority of long-term care hospitals for the elderly are still exposed to dangers.
Therefore, in this study, fire and evacuation simulations were performed using the fire occurrence time and horizontal refuge area designation as variables, and an evacuation safety evaluation was conducted.
According to the results,
1) Following the designation of the horizontal refuge areas, the RSET decreased at an average rate of 70% during the daytime (K hospital 55%, Y hospital 84%) and at an average rate of 77% at night (K hospital, 68%; Y hospital, 86%).
2) In cases where no horizontal refuge area was designated, the RSET increased at an average rate of 269% during the daytime (K hospital 123%, Y hospital 537%) and at an average rate of 412% at night (K hospital 215%, Y hospital 609%). That is, it was identified that in the case of a hospital with a high proportion of critically ill patients (Y hospital), horizontal refuge areas were more efficient./ The difference in the RSET between when horizontal refuge area were designated and when no horizontal refuge area was designated was larger at night when the number of workers was small.
3) When the horizontal refuge area was designated, it was found that evacuation safety was secured during both daytime and nighttime.
This study is meaningful in that it analyzes the efficiency of horizontal refuge areas in elderly care facilities by evaluating evacuation safety according to whether horizontal refuge areas are designated. The results of this study can be used as a basis for preparing retroactive provisions for the horizontal refuge areas in elderly care facilities. However, the simulations were conducted for only two long-term care hospitals for the elderly. Therefore, the results of this study have a limitation in that the method of designating the horizontal refuge area is limited to the target sites. Additional studies regarding the foregoing area are necessary.
Additional Remark
This paper was prepared by modifying and supplementing the first author’s manuscript(10) presented at the 2018 Fall Conference of the Korea Institute of Fire Science and Engineering.
Acknowledgment
This work was supported by the National Research Foundation of Korea (NRF) grant (No. NRF-2018R1A2B3005951), which was funded by the Korean government (MSIT) & This paper was supported by the “National Fire Agency” R&D program (20016433).